
Can I fall asleep during hypnotherapy and does it matter if I do?
The short answer is yes you can fall asleep during hypnotherapy! However, let’s explore why and when this might happen, and if it does, does it matter?
We know from the 6 stages of sleep (Dement & Kleitman, 1957), that when we go to bed and read for a few minutes before attempting sleep, we are likely to be in low beta. When we put the book down, turn off the lights and close our eyes, our brainwaves will descend from beta to alpha, to theta and finally, when we fall asleep, to delta.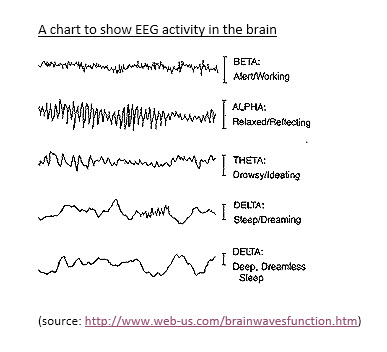
During stage 0 we are relaxed, with eyes closed but awake and there may be considerable tension in the body, and eyes move normally. The next stages, 1-4 are called quiet sleep, or slow-wave sleep because all of them are accompanied by slow brain waves, deep breathing, a calm and regular heartbeat, and reduced blood pressure.
As we drift from 0 into stage 1 our eyes move more slowly and begin to roll. The EEG frequency becomes irregular and alpha waves begin to disappear. The EEG pattern is actually very similar to the one that occurs when you are fully awake and mentally active.
After a few minutes in stage 1, we enter stage 2 sleep. In this stage, the EEG shows sharply pointed waves called sleep spindles. There are also special K-complexes, which are special waves with high peaks and deep valleys.
As we gradually enter stage 3 sleep, spindles and K-Complexes become more frequent but they are now mixed with delta waves, which are much slower and have a much higher amplitude (i.e. variations in height of the waves).
When delta waves occur more than 50% of the time, we have entered stage 4, the deepest level of sleep, from which it is most difficult to be aroused. It takes about ½ hour to reach stage 4 from stage 1 sleep.
REM (Rapid Eye Movement) Sleep
After 30-40 minutes in stage 4, a sleeper begins to retrace the journey, returning through stages 3, 2, then 1. Then begins a stage known as REM sleep or active sleep.
As in stage 1, the EEG during REM is similar to when we are active and awake, but now our heart rate, respiration, blood pressure and other physiological patterns also resemble those occurring during the day. At the same time, we begin rapid eye movements beneath closed lids.
Paradoxically, while brain waves and other measures resemble those of a person awake, muscle tone decreases to the point of virtual paralysis. Suddenly twitchy spasms appear, especially in the face and hands.
During the night most people travel up and down through these stages of sleep 4-6 times. Each complete cycle takes about 90 minutes. During the first half of the night, most time is spent in deeper sleep (stages 3 & 4) and only a few minutes in REM. The last half of the night is dominated by stage 2 and REM sleep, from which sleepers finally wake.
Here’s a summary of our typical cycle during sleep:

When an individual awakes from a deep sleep in preparation for getting up, their brainwave frequencies will increase through the different specific stages of brainwave activity. That is, they will increase from delta to theta and then to alpha and finally, when the alarm goes off, into beta. If that individual hits the snooze alarm button they will drop in frequency to a non-aroused state, or even into theta, or sometimes fall back to sleep in delta.
During this awakening cycle, it is possible for individuals to stay in the theta state for an extended period of say, five to 15 minutes. This would allow them to have a free flow of ideas about yesterday's events or to contemplate the activities of the forthcoming day. This time can be extremely productive and can be a period of very meaningful and creative mental activity.
Now this will make more sense hopefully in terms of the levels a hypnotherapist is aiming to achieve during a session to induce change at the subconscious level.
Hypnotherapy involves inducing a trance via hypnosis and delivering therapeutic interventions to help overcome the presenting issue e.g., lose weight, stop smoking, manage anxiety, cure a phobia, etc.
The alpha and theta stages are very useful to clients during the hypnotherapy session. It’s a period of activity, where the client is relaxing and reflecting, and processing creatively to find new ways of managing their issues better. To get there, however, clients need more or less time spent getting them from beta to alpha/theta stage because they either easily, or otherwise, find it difficult to relax.
Now there are many ways in which a trance can be induced, these ways can be long and relaxing, such as progressive relaxation, eye fixation, or guided imagery types inductions, or they can be very brief and surprising which distract the typical cognitive processing, such as physical or verbal requests which are unpredictable and unfamiliar to the person’s typical cognitive scripts e.g., eye roll and confusional inductions.
A hypnotherapist will choose the right style of induction for the person’s needs. So for example, someone who needs time to unwind, likes to feel an experience rather than just think it, needs to feel in control of their own experience and who needs to move at a pace comfortable for them, may enjoy a longer induction. This is different to someone who is impatient, where their mind wanders when they are not being stimulated cognitively, finds it ‘boring’ if they are not ‘doing’ something, or isn’t able to get in touch with their kinaesthetic modality very well, or simply doesn’t find longer inductions enjoyable. The latter may prefer to be induced quickly, leaving more perceived time for the therapy itself.
We know, however, that if we are left to our own devices for too long, are void of stimulation, and/or are very tired, the chances are we will fall asleep more quickly. So if a hypnotherapist fails to engage a client during the relaxed reflective stage of alpha, and the active creative processing stage of theta, and then expects a response from the client, the only response they are likely to receive is snoring!
This is the downside of using longer styles of inductions, or inductions without engagement, as they give the client plenty of time to skip past the beta and theta stages, deemed important to the process of change, and fall asleep!
To prevent this from happening, a well-trained hypnotherapist is aware of how deep a client is experiencing trance, and will check in regularly with the client and use their sensory acuity to lighten trance at the appropriate stages to ensure that the presenting issue is being dealt with 'actively' and effectively.
With regards to whether it matters if a client falls asleep, this typically depends largely on the client and their beliefs. If a client believes that they are still absorbing information during the deeper stages of sleep and that by being completely unaware of what is happening during a session, they will still achieve the desired benefit, the chances are they will!
On the other hand, if a client’s belief is that because they were completely unaware during the session and so presumed they had fallen asleep, and in their mind, nothing seems to happen during sleep, and they will have wasted their time and money being there, they probably won’t get the expected change they desire!
A client can, however, erroneously believe they have fallen asleep because they’ve had amnesia during the session. Amnesia, however, is a hypnotic phenomenon and a sign that the client has been in trance i.e., actively focusing on some things at the exclusion of others. The difference is that if the client is able to respond to requests from the hypnotherapist, albeit in a delayed way, they haven't ‘fallen asleep’.
If the client is unable to respond or disengage from trance relatively quickly on request from the hypnotherapist, and they are heavily snoring and unaware of it, the chances are they were allowed to ‘fall asleep'!
References
Dement, W., & Kleitman, N. (1957) 'Cyclic variations in EEG during sleep and their relation to eye movements, body motility, and dreaming'. Electroencephalography and Clinical Neurophysiology, 9: 673-690.
Horne, J.A. (2000) REM sleep – by default? Neuroscience and Biobehavioural Reviews, 24: 777-797.
NyKamp, K., Rosenthal, L., Folkerts, M., Roehrs, T., Guido, P., & Roth, T. (1998) 'The effects of REM sleep deprivation on the level of sleepiness/alertness'. Sleep 21: 609-614.
Pinel, J., P., J. (2006) Biopsychology. (6th Edition). Boston: Allyn and Bacon.
Rechtschaffen, A. (1998) 'Current perspectives on the function of sleep'. Perspectives in Biology and Medicine, 41: 359-390.




